A Double-Blind Randomized Clinical Trial
Key Points
Question What quantifiable differences exist between botulinum toxin A formulations when used for cosmetic treatment in the glabella?
Findings In this randomized clinical trial of 143 adult female individuals, abobotulinum toxin A and prabotulinum toxin A displayed the most rapid onset, and incobotulinum toxin A and prabotulinum toxin A exhibited lasting effect at 180 days. Prabotulinum toxin A exhibited a significantly greater effect at 180 days than onabotulinum toxin A, but all formulations resulted in significant improvement in strain and patient satisfaction up to 90 days.
Meaning The trial results suggest that there are distinct and measurable clinical and patient-reported outcome differences between botulinum toxin A formulations that may be considered when evaluating a patient’s aesthetic goals.
Abstract
Comparison of Botulinum Toxin A Formulations for Glabellar Strain Treatment in Women
Importance Multiple botulinum toxin A formulations were approved by the US Food and Drug Administration for treating the glabellar rhytids. A comparative quantitative evaluation of their effects on the glabella has not been conducted.
Objective To provide an objective quantitative assessment of the effect of 4 botulinum toxin A formulations on glabellar strain across using dynamic 3-dimensional photogrammetry.
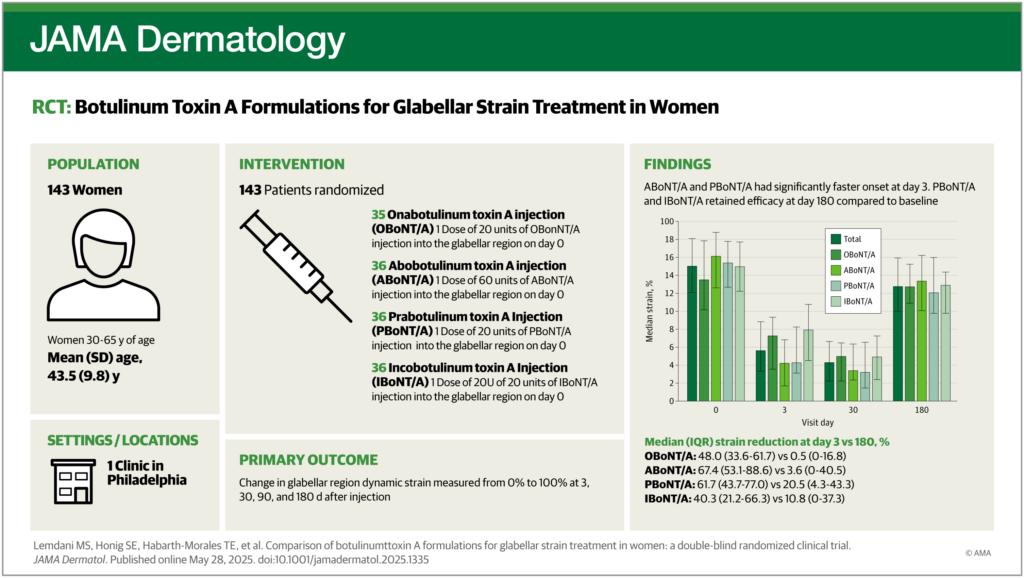
Design, Setting, and Participants This single-center, double-blind clinical trial, conducted at the University of Pennsylvania Division of Plastic Surgery clinic, randomized 143 female individuals aged 30 to 65 years into 4 arms receiving different botulinum toxin A formulations on day 0 and with follow-up at days 3, 30, 90, and 180. Dynamic 3-dimensional photogrammetry and surveys were collected from March 2022 to June 2023 and analyzed from July 2023 to April 2024.
Interventions Participants were randomized 1:1:1:1 into 4 treatment arms: 1 dose of 20 units of onabotulinum toxin A (OBoNT/A); 1 dose of 50 units of abobotulinum toxin A (ABoNT/A); 1 dose of 20 units of prabotulinum toxin A (PBoNT/A); or 1 dose of 20 units of incobotulinum toxin A (IBoNT/A) into the glabellar region (GR).
Main Outcomes and Measures The primary outcome was change in GR dynamic strain after injection over time. Secondary outcomes included changes in patient-reported satisfaction, the relationship between baseline strain severity and postinjection improvement in strain, and the effect on the strain of the untreated lateral canthal region.
Results This study recruited 143 female individuals with a mean (SD) age of 43.5 (9.8) years. ABoNT/A and PBoNT/A had the fastest onset at day 3. PBoNT/A and IBoNT/A retained efficacy at day 180 compared with their baseline. Increasing baseline glabellar strain severity resulted in increased improvement with treatment. Lateral canthal region strain increased with decreasing GR strain. PBoNT/A was significantly more effective at day 180 than OBoNT/A. All arms experienced improvement in related FACE-Q module scores up to 90 days.
Conclusions and Relevance This randomized clinical trial found that ABoNT/A and PBoNT/A displayed the most rapid onset of effect. The peak effect is similar across all toxins. When measuring strain at approximately 6 months, some toxins remain significant relative to their own baseline or compared with other specific toxins.
Trial Registration ClinicalTrials.gov Identifier: NCT05167864
Introduction
Botulinum toxin type A (BoNT/A) injection is the most common aesthetic intervention in the US, experiencing a 73% increase to more 8.7 million procedures in 2022.1 The US Food and Drug Administration (FDA) has approved 5 additional BoNT/A formulations beyond the original onabotulinum toxin A (OBoNT/A), including abobotulinum toxin A (ABoNT/A), incobotulinum toxin A (IBoNT/A), prabotulinum toxin A (PBoNT/A), daxibotulinum toxin A (DBoNT/A), and letibotulinum toxin A (LBoNT/A) for the glabellar region (GR).2–6 Despite a common enzymatically active light chain (LC) molecule, each neurotoxin should be considered individually due to their unique manufacturing process and variations in preparation, resulting in distinct clinical features.7,8
Comparisons between formulations of BoNT/A have been conducted; however, few have used precise, objective metrics. Validated scales have assessed rhytids of facial regions after BoNT/A injection.9–14 However, scales categorize subjective observations, resulting in indirect assessments and bias, preventing the granularity offered through tools like dynamic 3-dimensional (3D) imaging.
Several studies have integrated objective measurements into assessment of BoNT/A efficacy. Three-dimensional imaging has been successfully used to measure static and dynamic rhytids.15,16 These studies serve as a small but important growing body of literature implementing 3D imaging in aesthetic studies.17–20 Wilson et al21 successfully used 3D imaging in 2016 to study the effect of dynamic strain across 3 types of BoNT/A. Their findings used digital image correlation and dynamic tissue strain to quantify the dynamic rhytid and effect of BoNT/A, validating the application of the technology in comparative aesthetic research.21–23
With novel BoNT/A formulations and improvement in digital image technology, it is critical to precisely measure different BoNT/A clinical outcomes to advance our understanding of these treatments. No studies have specifically compared treatment results with patient-reported outcomes (PROs).24–28 This work aimed to perform a double-blind, prospective, randomized clinical trial to compare 4 different BoNT/A formulations (OBoNT/A, ABoNT/A, PBoNT/A, and IBoNT/A) using digital image correlation to precisely quantify the effect of 4 toxins on the GR relative to PROs.
Methods
This study was approved by the University of Pennsylvania institutional review board and registered on ClinicalTrials.gov (NCT05167864) (Supplement 1). A total of 143 female patients provided written consent to participate in this trial conducted at a Penn Medicine plastic surgery clinic. Inclusion criteria included being female, age between 30 and 65 years, any Fitzpatrick skin type, Glogau score, or rhytid severity. Exclusion criteria included being male, glabellar injection for the rhytids within 12 months before the study, surgery above the malar region, and any condition affecting facial expression. Block randomization was used to randomly assign participants into each study arm using REDCap electronic data capture tools initiated by one of the authors (R.B.B.). The computer-generated random sequence was produced by one of the authors (R.B.B.) using the Research Randomizer.29 REDCap conducts randomization as participants are recruited, and this process was obscured to the authors.30 ,31 Forty blocks of 4 assignments per block were used until study enrollment was complete. Patients received treatment on day 0 and were requested to follow up at days 3 ± 1, 30 ± 5, day 90 ± 7, and 180 ± 10 (Figure 1). Treatment was administered by a single, masked plastic surgeon (I.P.) according to FDA-approved guidelines. Separate preparation of each treatment was performed by other clinicians, with multiple employed to prevent any from knowing the treatment number or order. Participants were masked to the formulation received. Treatment arms consisted of 1:1:1:1 ratios of OBoNT/A (Botox; Allergan), ABoNT/A (Dysport; Ipsen Biopharmaceuticals Inc), PBoNT/A (Jeuveau; Evolus), and IBoNT/A (Xeomin; Merz Pharmaceuticals). Participants in the OBoNT/A, PBoNT/A, and IBoNT/A arms received a standardized dosage of 20 units, with 4 units administered at 5 standard sites in the GR, while ABoNT/A participants received 50 units administered in the same pattern.32 Reconstitutions were performed with 2.5 mL of sterile saline per 100 units (OBoNT/A, PBoNT/A, IBoNT/A) or 3.0 mL per 300 unit (ABoNT/A) vial and each injection point was treated with 0.1 mL of product. LBoNT/A (Letybo; Hugel) and DBoNT/A (Daxxify; Revance Therapeutics) were excluded as their FDA approvals were given after the trial’s initiation. This study followed the Consolidated Standards of Reporting Trials (CONSORT) reporting guidelines.
Figure 1. CONSORT Flow Diagram
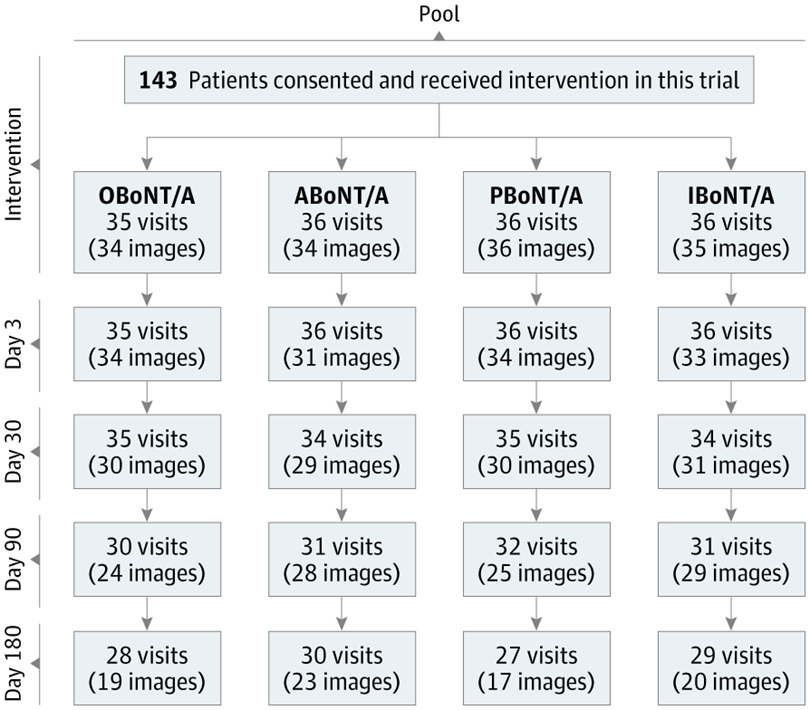
Visits refers to number of patients who arrived at each visit day. Images refer to the number of patients who had successful 3-dimensional images that could be incorporated into the analysis. ABoNT/A indicates abobotulinum toxin A; IBoNT/A, incobotulinum toxin A; OBoNT/A, onabotulinum toxin A; PBoNT/A, prabotulinum toxin A.
At each visit, 2 images were captured, neutral and dynamic. The neutral face was relaxed and served as a reference while the dynamic face was the expression when asked to furrow the glabella. Three-dimensional photogrammetry was performed using the VECTRA M3 (Canfield Scientific, Inc) to allow for dynamic measurements of facial strain. The photographs were rendered as a 3D mesh that was composed of interconnecting points. Multiple theoretical circles, formed by the interconnection of the mesh’s points, are formed and can be compressed when those points approach each other during furrowing. Strain was defined as the percentage difference in the length of the theoretical circle’s shortest axis between the neutral and dynamic face. The result was a heatmap that reflected the precise quantification of the region and served as an effective measure of the effect of BoNT/A. Each participant had a median strain value for the GR. For the cohort and each treatment arm, the median strain value at each visit was determined. A post hoc analysis of these photographs repeated this process to measure lateral canthal region (LCR) strain.
Baseline photography and FACE-Q surveys were captured preinjection on day 0. Postintervention photography was performed at follow-up visits. The FACE-Q was administered electronically to participants at each visit independently of image capture.33 Focus was given to the 5 GR-related FACE-Q modules, specifically “appraisal of lines: forehead,” “satisfaction with forehead and eyebrows,” “appraisal of lines: between eyebrows,” “satisfaction with eyes,” and “satisfaction with facial appearance.”
The sample size was based on a previously successful similar study and had an anticipated 30% dropout.21 The measured outcome was the change in dynamic strain in the glabella area after injection over time. Effect size was taken from this to be a Cohen d of 0.85. Due to an increase in the number of follow-up visits for this study, we increased the participant population to account for an increased dropout. With a power of 80%, α level of .05, and expected dropout rate of 30%, 32 participants were required for each group.
The intention-to-treat principle was applied for analysis due to some participants missing follow-up visits. Missing data, namely any missed follow-up visits, were excluded from analysis. Categorical demographic data were represented with frequencies and continuous with means and standard deviations. Normalized strain values were calculated by dividing the strain value at each posttreatment visit by the baseline strain value and expressing this result as a percentage. A paired t test was used when a Shapiro-Wilk test had a P value of greater than .05 and parametric assumptions were met; however, Wilcoxon signed rank tests were conducted when a Shapiro-Wilk test had a P value of less than .05. GR and LCR strain values were compared with their baseline at day 0 to determine improvement from baseline. This analysis was also conducted for each FACE-Q module. Baseline glabellar strain was placed into severity quartiles and compared with MTE to assess the relationship between strain severity and the degree of improvement via linear regression. A linear mixed-effects model was used to assess the relationship between strain and survey scores throughout the treatment period. Photogrammetry analysis and strain value generation were conducted by Canfield Scientific, Inc. A 2-tailed P value of <.05 was considered significant. The analysis was conducted with R, version 4.4.1 (R Foundation for Statistical Computing).34
Results
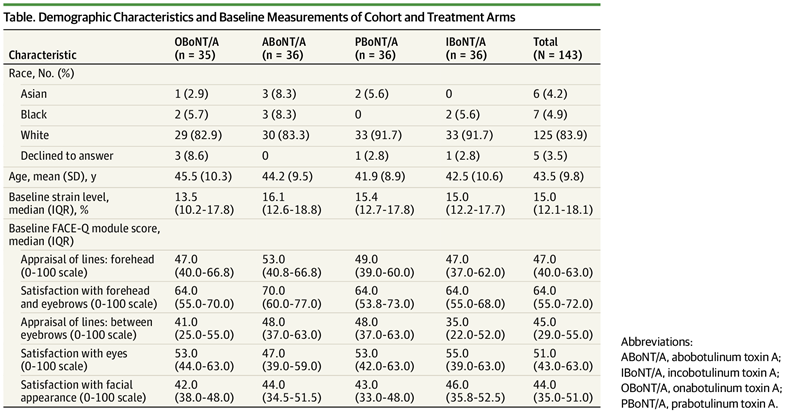
A total of 143 participants were randomized to 1 of 4 treatment arms. No participants withdrew from the trial. No participants experienced an adverse event. Four participants were completely excluded due to poor imaging results at pretreatment (Figure 1). Excluded visits included when participants did not return or when there were poor imaging results on follow-up. Demographic characteristics between the arms were similar, and all participants were female to avoid sex difference in response to BoNT/A (Table).35
Table. Demographic Characteristics and Baseline Measurements of Cohort and Treatment Arms
Relative to pretreatment strain levels, on day 0, a significant decrease in strain was observed at every visit date except day 180 for OBoNT/A and ABoNT/A (Figure 2B). The relative median change in strain at each posttreatment point was also measured between arms. ABoNT/A (67.4%; IQR, 53.1%-88.6% reduction) had a significantly faster onset in relative strain reduction at day 3 than OBoNT/A (48.0%; IQR, 33.6%-61.7%; P = .001) and IBoNT/A (40.3%; IQR, 21.2%-66.3%; P = .002). PBoNT/A (61.7%; IQR, 3.7%-77.0%) also had a faster onset than OBoNT/A and IBoNT/A. Finally, PBoNT/A strain reduction (20.5%; IQR, 4.3%-43.3%) was significantly higher than OBoNT/A at day 180 (0.5%; IQR, 0%-16.8%; P = .03). No other measurements were significant (Figure 2C).
Figure 2. Distribution, Value, and Reduction in Strains
A, Distribution of strain in glabellar (GLAB) region and lateral canthal region (LCR) in 1 participant. B, GLAB strain value by toxin type at each study visit (n = 139). C, Comparison of relative reduction in strain across treatment arms at each visit (n = 139). ABoNT/A indicates abobotulinum toxin A; IBoNT/A, incobotulinum toxin A; LLCL, left lateral canthal lines; OBoNT/A, onabotulinum toxin A; PBoNT/A, prabotulinum toxin A; RLCL, right lateral canthal lines.
aB, Significant at P < .05 with day 0 as reference. C, Significantly reduced strain to OBoNT/A and IBoNT/A on same visit day at P < .05.
bSignificantly reduced strain to OBoNT/A on same visit day at P < .05.
The percentage of maximum treatment efficacy (MTE) at each visit was examined within the cohort and arms to better delineate onset and duration (eFigure 1 in Supplement 2). MTE occurred most often at day 30, with a median efficacy of 88% in the total cohort, 89.3% in the OBoNT/A, 93% in the PBoNT/A, and 89.5% in the IBoNT/A arms. Between all arms, none showed a significant difference at day 30. MTE for ABoNT/A occurred at day 3 at 85.3% and maintained similar efficacy on day 30 at 80.1%. Onset at day 3 for the other arms varied, including 70.4% for OBoNT/A, 81.8% for PBoNT/A, and 64.1% for IBoNT/A. The ABoNT/A treatment efficacy was significantly higher at onset than OBoNT/A and IBoNT/A, and PBoNT/A was faster at onset than IBoNT/A. Day 90 demonstrated no significant differences in effect between the arms. At day 180, PBoNT/A was significantly higher than OBoNT/A, although no other arms were significantly different from each other.
The relationship between MTE and baseline strain was further assessed. The study cohort was divided into quartiles by strain severity in which the lowest strain quartile was used as the reference. A significant increase in strain improvement was revealed that continued to increase with each successive strain severity quartile (eFigure 3 in Supplement 2). This relationship persisted across arms, with almost every quartile exhibiting significant increases in strain improvement relative to the lowest quartile (eFigure 3 in Supplement 2).
A post hoc analysis of strain in the untreated LCR was conducted in the total cohort to assess potential strain recruitment in the adjacent untreated periorbit (Figure 3). LCR strain increased significantly at days 3 and 30 compared with baseline strain. However, by day 90, and by extension day 180, LCR strain was similar to day 0. This trend was inverse to glabellar strain. However, LCR strain returned to baseline by day 90, while glabellar strain remained significantly reduced.
Figure 3. Lateral Canthal Region Strain at Each Visit for All 139 Participants
aSignificant at P < .05 with day 0 as reference.
FACE-Q module scores demonstrated a significant increase from day 0 across 5 GR modules at every follow-up visit relative to baseline, demonstrating improved participant satisfaction that correlated with the strength of the effect across all 6 months of the study (eFigure 2 in Supplement 2). FACE-Q scores in these modules across arms were also assessed (eFigure 2 in Supplement 2). Generally, all arms had significant improvements in module scores at day 30, with a minority losing significance at days 90 or 180 (eFigure 2 in Supplement 2). When comparing differences between arms at each visit day, no differences were elicited in any of the FACE-Q module scores (eTable 1 in Supplement 2).
The correlation between strain and PRO scores throughout the treatment period was also assessed for the total cohort and within each treatment arm (eTable 2 in Supplement 2). Each relationship showed a clear and significant inverse correlation between strain and PRO scores for most modules, with the most relevant module, “appraisal of lines: between eyebrows,” showing the largest quantified association between strain and FACE-Q scores for all arms.
Discussion
Since its introduction by our group in 2014 and an initial comparative BoNT/A analysis in 2016, digital image correlation (DIC) has substantially improved via reduced image collection time and more precise and reproducible measurements.20,21,36 Thus, DIC has revealed specific, clinically relevant differences between 4 BoNT/A formulations.20 By standardizing dosage administration, we examined each formulation’s unique effects via different and complementary analyses with minimal confounders.37–42
Overall, the results demonstrated that all BoNT/A formulations significantly reduced GR strain, which was consistent with studies that used varied methods to evaluate glabellar rhytid correction, including DIC, electromyography, and subjective scoring.4,11,25,43–45 These results further underscore that the differentiation of formulations requires precise evaluation of characteristics beyond the peak effect.
As such, we evaluated neurotoxins at 4 points and demonstrated specific differences in onset and duration. Consistent with prior studies, ABoNT/A and PBoNT/A demonstrated the most rapid onset relative to baseline and MTE.27 The difference in onset was significant relative to the OBoNT/A and IBoNT/A cohorts, although ABoNT/A and PBoNT/A did not differ significantly from each other. Thus, either ABoNT/A or PBoNT/A may be considered when a faster onset is desired. At peak effect, the 4 neurotoxins were not statistically different from one another, as observed in a prior study of the masseters.46
All toxin formulations retain significant correction of glabellar strain for up to 3 months with on-label dosing, and few BoNT/A studies have examined the effect after 3 months. PBoNT/A and IBoNT/A maintained significant strain correction at day 180 relative to baseline. These data extend beyond those of a study comparing OBoNT/A to PBoNT/A that demonstrated that 20 units of either toxin resulted in approximately 150 days of effect duration by investigator assessment.47 However, this retained improvement’s significance relative to other toxins may be limited, as PBoNT/A was only significantly greater than OBoNT/A, while IBoNT/A showed no significant difference to other toxins. These results suggest that practitioners may prefer ABoNT/A or PBoNT/A for patients seeking rapid onset, while PBoNT/A may also provide longer-lasting effects in some cases. These findings are consistent with anecdotal evidence and potentially provide a quantitative foundation for clinical decisions.
Response rates to BoNT/A vary between individuals.21,42,48–50 A prior study of BoNT/A efficacy distinguished participants with significant response from those without.47 To further examine individual responses to BoNT/A, we evaluated the baseline strain relative to MTE. The data demonstrated that individuals with more severe baseline strain also experienced more significant strain reduction with on-label dosing. This finding suggests that strong pretreatment glabellar strain may not require more dosing for adequate correction and further underscores the importance of educating patients with robust glabellar strain about static vs dynamic rhytid etiology.
Multiple studies have demonstrated that participant satisfaction outcomes are met with BoNT/A treatment, up to and exceeding 4 months.4,14,51–58 Our cohort and all arms demonstrated significant improvement in satisfaction in 5 GR-related modules. Significantly, satisfaction was correlated with glabellar strain correction, suggesting first that participants’ perception of treatment effect was accurate, second that effect was correlated with satisfaction, and third that glabellar improvement also resulted in perceived improvement of adjoining areas of the face. In particular, the “appraisal of lines: between eyebrows” module demonstrated the greatest improvement and maintained significance at day 180 in the OBoNT/A, PBoNT/A, and IBoNT/A arms, although not the ABoNT/A arm. This aligned with the analysis between this module’s relationship to change in strain, as further demonstrated by the PBoNT/A and IBoNT/A arms. In these arms, this subjective improvement corresponded with objective strain improvement, as both had significant treatment duration at day 180. Additional modules that retained significance from baseline at day 180 varied across arms, indicating that, although participants noted reduction in BoNT/A efficacy, there was some perceptible retained effect at 6 months. PRO data demonstrated long-lasting satisfaction with GR neuromodulation that was correlated with treatment effects.
Our examination of the LCR assessed dynamic recruitment in the periorbital region outside the treated area to test the hypothesis that reduced glabellar activity results in increased activity (strain) in the LCR as a compensatory mechanism.59 The significant increase in LCR strain at days 3 and 30, which corresponded to onset and maximum GR strain reduction, suggests a dynamic relationship between neighboring anatomic regions during facial expression and that the treatment of one region affects another’s activity.
Limitations
Our study had several limitations. Participant retention, specifically at the last study visit, was reduced. Only female individuals were included in the study, and the results may not be directly extrapolated to male individuals. Differential dosing and treatment of adjoining regions could not be examined due to institutional board review restrictions and financial constraints. The LCR analysis was post hoc; thus, it was more limited than the GR analysis. Further, depending on the variables, we chose to use paired t tests, Wilcoxon signed-rank tests, or linear regression models for comparisons across arms without adjusting for multiplicity. This approach preserves statistical power and highlights clinically relevant trends, such as the faster onset and longer duration. While we acknowledge the potential for type 1 errors, our findings were consistent with prior studies and potentially provide meaningful guidance for clinical practice. Despite these limitations, to our knowledge, this study was the largest double-blinded, randomized clinical trial examining the effectiveness of 4 BoNT/A formulations in the GR. The use of 3D photogrammetry for precise, objective measurements underscores the rigor of this work.9 Future studies are recommended to apply 3D photogrammetry to assess differential BoNT/A dosing, reconstitution, and dispersion rates to expand our understanding of the clinical effect of varied BoNT/A formulations.
Conclusions
This randomized clinical trial demonstrated precise quantitative differences between 4 BoNT/A formulations in treating glabellar strain with significant clinical implications. ABoNT/A and PBoNT/A demonstrated significantly faster onset than OBoNT/A or IBoNT/A. PBoNT/A retained a significant effect at day 180 relative to baseline and compared with OBoNT/A, while IBoNT/A retained a significant effect at day 180 compared with the baseline. Quantification of BoNT/A effect provides an objective foundation to guide individualized product selection and patient education.
Article Information
Accepted for Publication: March 29, 2025.
Published Online: May 28, 2025. doi:10.1001/jamadermatol.2025.1335
Corresponding Author: Ivona Percec, MD, PhD, Perelman Center for Advanced Medicine, 3400 Civic Center Blvd, 14th Floor, Philadelphia, PA 19104 (ivona.percec@pennmedicine.upenn.edu).
Correction: This article was corrected on August 20, 2025, to fix errors in the Methods section.
Author Contributions: Drs Percec and Serletti had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis.
Concept and design: Lemdani, Habarth-Morales, Davis, Broach, Serletti, Percec.
Acquisition, analysis, or interpretation of data: All authors.
Drafting of the manuscript: Lemdani, Honig, Habarth-Morales, Broach, Serletti.
Critical review of the manuscript for important intellectual content: All authors.
Statistical analysis: Lemdani, Honig, Habarth-Morales, Broach.
Obtained funding: Broach, Percec.
Administrative, technical, or material support: Honig, Davis, Niu, Broach, Percec.
Supervision: Davis, Broach, Serletti, Percec.
Conflict of Interest Disclosures: Drs Lemdani, Broach, and Davis reported grants from Evolus during the conduct of the study. Dr Percec reported grants from Evolus during the conduct of the study as well as personal fees from AbbVie and Galderma outside the submitted work. No other disclosures were reported.
Funding/Support: Evolus, manufacturer of Jeuveau (prabotulinumtoxinA), provided funding via an investigator-initiated trial grant. In addition to direct funding for the trial, the grant was also used to fund Canfield Scientific, Inc, who generated quantified data from photographs collected during the trial.
Role of the Funder/Sponsor: The funding organizations had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Data Sharing Statement: See Supplement 3.
Additional Contributions: We thank the patient in Figure 2 for granting permission to publish this information.
Additional Contributions: We thank Kyle Seid, BS, and Benjamin Altieri, BS, of the statistical analysis team at Imalogix for consultation on statistical analysis for this trial. These individuals were not compensated for their contributions.
References
1.American Society of Plastic Surgeons. Plastic surgery statistics. Accessed May 3, 2024. https://www.plasticsurgery.org/news/plastic-surgery-statistics
2.Glogau R, Kontis TC, Liu Y, Gallagher CJ. Progressive improvement in static glabellar lines after repeated treatment with daxibotulinumtoxina for injection. Dermatol Surg. 2021;47(12):1579-1584. doi:10.1097/DSS.0000000000003211PubMedGoogle ScholarCrossref
3.Gold M, Taylor S, Mueller DS, et al. Efficacy and safety of letibotulinumtoxina in the treatment of moderate and severe glabellar lines in females 35 to 50 years of age: post hoc analyses of the phase 3 clinical study data. Aesthet Surg J Open Forum. 2024;6:ojae010. doi:10.1093/asjof/ojae010PubMedGoogle ScholarCrossref
4.Vasile G, Green C, Bhatti H, et al. OnabotulinumtoxinA versus prabotulinumtoxinA-xvfs: a randomized, triple-blind, split-face study on the time to onset, rhytid appearance, and patient satisfaction in forehead and glabellar 9lines. J Clin Aesthet Dermatol. 2023;16(5):47-49.PubMedGoogle Scholar
5.Kerscher M, Fabi S, Fischer T, et al. IncobotulinumtoxinA demonstrates safety and prolonged duration of effect in a dose-ranging study for glabellar lines. J Drugs Dermatol. 2020;19(10):985-991. doi:10.36849/JDD.2020.5454PubMedGoogle ScholarCrossref
6.Han X, Bai J, Kuang J. Efficacy and safety of abobotulinumtoxinA for treatment of moderate-to-severe glabellar lines: a meta-analysis. Ophthalmic Plast Reconstr Surg. 2024;40(2):126-133. doi:10.1097/IOP.0000000000002491PubMedGoogle ScholarCrossref
7.Brodsky MA, Swope DM, Grimes D. Diffusion of botulinum toxins. Tremor Other Hyperkinet Mov (N Y). 2012;2:tre-02-85-417-1.PubMedGoogle Scholar
8.Samizadeh S, De Boulle K. Botulinum neurotoxin formulations: overcoming the confusion. Clin Cosmet Investig Dermatol. 2018;11:273-287. doi:10.2147/CCID.S156851PubMedGoogle ScholarCrossref
9.Flynn TC, Carruthers A, Carruthers J, et al. Validated assessment scales for the upper face. Dermatol Surg. 2012;38(2 Spec No.):309-319. doi:10.1111/j.1524-4725.2011.02248.xPubMedGoogle ScholarCrossref
10.Roberts WE, Miller N. Optimized patient outcomes with the novel modality of corrective chemical peel and neurotoxin on same-day treatment. J Drugs Dermatol. 2024;23(1):1349-1354. doi:10.36849/JDD.7194PubMedGoogle ScholarCrossref
11.Yeilding RH, Fezza JPA. A prospective, split-face, randomized, double-blind study comparing onabotulinumtoxinA to incobotulinumtoxinA for upper face wrinkles. Plast Reconstr Surg. 2015;135(5):1328-1335. doi:10.1097/PRS.0000000000001255PubMedGoogle ScholarCrossref
12.Baumann L, Dayan S, Connolly S, et al. Duration of clinical efficacy of onabotulinumtoxinA in crow’s feet lines: results from two multicenter, randomized, controlled trials. Dermatol Surg. 2016;42(5):598-607. doi:10.1097/DSS.0000000000000757PubMedGoogle ScholarCrossref
13.Prager W, Bee EK, Havermann I, Zschocke I. Onset, longevity, and patient satisfaction with incobotulinumtoxinA for the treatment of glabellar frown lines: a single-arm, prospective clinical study. Clin Interv Aging. 2013;8:449-456. doi:10.2147/CIA.S34854PubMedGoogle ScholarCrossref
14.Rivers JK, Bertucci V, McGillivray W, et al. Subject satisfaction with onabotulinumtoxinA treatment of glabellar and lateral canthal lines using a new patient-reported outcome measure. Dermatol Surg. 2015;41(8):950-959. doi:10.1097/DSS.0000000000000424PubMedGoogle ScholarCrossref
15.Rappl T, Wurzer P, May S, et al. Three-dimensional evaluation of static and dynamic effects of botulinum toxin A on glabellar frown lines. Aesthetic Plast Surg. 2019;43(1):206-212. doi:10.1007/s00266-018-1230-yPubMedGoogle ScholarCrossref
16.Lumenta DB, Selig H, Kitzinger HB, Kamolz LP. Objective quantification of wrinkles: three-dimensional analysis of surface irregularity. Plast Reconstr Surg. 2012;129(4):735e-737e. doi:10.1097/PRS.0b013e318245e74ePubMedGoogle ScholarCrossref
17.Chang CS, Chang BL, Lanni M, Wilson AJ, Beer J, Percec I. Perioral rejuvenation: a prospective, quantitative dynamic three-dimensional analysis of a dual modality treatment. Aesthet Surg J. 2018;38(11):1225-1236. doi:10.1093/asj/sjy060PubMedGoogle ScholarCrossref
18.Percec I, Bertucci V, Solish N, Wagner T, Nogueira A, Mashburn J. An objective, quantitative, dynamic assessment of hyaluronic acid fillers that adapt to facial movement. Plast Reconstr Surg. 2020;145(2):295e-305e. doi:10.1097/PRS.0000000000006461PubMedGoogle ScholarCrossref
19.Schlager S, Kostunov J, Henn D, Stark BG, Iblher N. A 3D morphometrical evaluation of brow position after standardized botulinum toxin A treatment of the forehead and glabella. Aesthet Surg J. 2019;39(5):553-564. doi:10.1093/asj/sjy205PubMedGoogle ScholarCrossref
20.Kwon IJ, Lee W, Moon HJ, Lee SE. Dynamic evaluation of skin displacement by the frontalis muscle contraction using three-dimensional skin displacement vector analysis. Yonsei Med J. 2023;64(7):440-447. doi:10.3349/ymj.2022.0605PubMedGoogle ScholarCrossref
21.Wilson AJ, Chang B, Taglienti AJ, et al. A quantitative analysis of onabotulinumtoxinA, abobotulinumtoxinA, and incobotulinumtoxinA: a randomized, double-blind, prospective clinical trial of comparative dynamic strain reduction. Plast Reconstr Surg. 2016;137(5):1424-1433. doi:10.1097/PRS.0000000000002076PubMedGoogle ScholarCrossref
22.Wilson AJ, Chin BC, Hsu VM, Mirzabeigi MN, Percec I. Digital image correlation: a novel dynamic three-dimensional imaging technique for precise quantification of the dynamic rhytid and botulinum toxin type a efficacy. Plast Reconstr Surg. 2015;135(5):869e-876e. doi:10.1097/PRS.0000000000001224PubMedGoogle ScholarCrossref
23.Chang BL, Wilson AJ, Taglienti AJ, Chang CS, Folsom N, Percec I. Patient perceived benefit in facial aesthetic procedures: FACE-Q as a tool to study botulinum toxin injection outcomes. Aesthet Surg J. 2016;36(7):810-820. doi:10.1093/asj/sjv244PubMedGoogle ScholarCrossref
24.Kundu N, Kothari R, Shah N, et al. Efficacy of botulinum toxin in masseter muscle hypertrophy for lower face contouring. J Cosmet Dermatol. 2022;21(5):1849-1856. doi:10.1111/jocd.14858PubMedGoogle ScholarCrossref
25.Bonaparte JP, Ellis D, Quinn JG, Rabski J, Hutton B. A comparative assessment of three formulations of botulinum toxin type A for facial rhytides: a systematic review with meta-analyses. Plast Reconstr Surg. 2016;137(4):1125-1140. doi:10.1097/PRS.0000000000002004PubMedGoogle ScholarCrossref
26.Prager W, Nogueira Teixeira D, Leventhal PS. Incobotulinumtoxina for aesthetic indications: a systematic review of prospective comparative trials. Dermatol Surg. 2017;43(7):959-966. doi:10.1097/DSS.0000000000001076PubMedGoogle ScholarCrossref
27.Nestor M, Cohen JL, Landau M, et al. Onset and duration of abobotulinumtoxinA for aesthetic use in the upper face: a systematic literature review. J Clin Aesthet Dermatol. 2020;13(12):E56-E83.PubMedGoogle Scholar
28.Rahman E, Mosahebi A, Carruthers JDA, Carruthers A. The efficacy and duration of onabotulinum toxin A in improving upper facial expression lines with 64-unit dose optimization: a systematic review and meta-analysis with trial sequential analysis of the randomized controlled trials. Aesthet Surg J. 2023;43(2):215-229. doi:10.1093/asj/sjac253PubMedGoogle ScholarCrossref
29.Urbaniak GC, Plous S. Research randomizer (version 4.0). Accessed November 2, 2023. https://www.randomizer.org/
30.Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)–a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009;42(2):377-381. doi:10.1016/j.jbi.2008.08.010PubMedGoogle ScholarCrossref
31.Harris PA, Taylor R, Minor BL, et al; REDCap Consortium. The REDCap consortium: building an international community of software platform partners. J Biomed Inform. 2019;95:103208. doi:10.1016/j.jbi.2019.103208PubMedGoogle ScholarCrossref
32.US Food and Drug Administration. Drugs@FDA: FDA-approved drugs. Accessed January 20, 2025. https://www.accessdata.fda.gov/scripts/cder/daf/index.cfm?event=overview.process&ApplNo=103000
33.Klassen AF, Cano SJ, Schwitzer JA, et al. Development and psychometric validation of the FACE-Q skin, lips, and facial rhytids appearance scales and adverse effects checklists for cosmetic procedures. JAMA Dermatol. 2016;152(4):443-451. doi:10.1001/jamadermatol.2016.0018
ArticlePubMedGoogle ScholarCrossref
34.R Core Team. R: A Language and Environment for Statistical Computing. R Foundation for Statistical Computing; 2024.
35.Nestor MS, Arnold D, Fischer DL. The mechanisms of action and use of botulinum neurotoxin type A in aesthetics: key clinical postulates II. J Cosmet Dermatol. 2020;19(11):2785-2804. doi:10.1111/jocd.13702PubMedGoogle ScholarCrossref
36.Hsu VM, Wes AM, Tahiri Y, Cornman-Homonoff J, Percec I. Quantified facial soft-tissue strain in animation measured by real-time dynamic 3-dimensional imaging. Plast Reconstr Surg Glob Open. 2014;2(9):e211. doi:10.1097/GOX.0000000000000185PubMedGoogle ScholarCrossref
37.Bertucci V, Green JB, Fezza JP, Brown J, Gallagher CJ, Solish N. Impact of glabellar injection technique with daxibotulinumtoxina for injection on brow position. Aesthet Surg J. 2023;43(suppl 1):S10-S18. doi:10.1093/asj/sjac002PubMedGoogle ScholarCrossref
38.Sung Y, Nam SM, Lew H. Clinical outcomes of individualized botulinum neurotoxin type A injection techniques in patients with essential blepharospasm. Korean J Ophthalmol. 2015;29(2):115-120. doi:10.3341/kjo.2015.29.2.115PubMedGoogle ScholarCrossref
39.Hong SO. Cosmetic treatment using botulinum toxin in the oral and maxillofacial area: a narrative review of esthetic techniques. Toxins (Basel). 2023;15(2):82. doi:10.3390/toxins15020082PubMedGoogle ScholarCrossref
40.Polacco MA, Singleton AE, Barnes CH, Maas C, Maas CSA. A double-blind, randomized clinical trial to determine effects of increasing doses and dose-response relationship of incobotulinumtoxinA in the treatment of glabellar rhytids. Aesthet Surg J. 2021;41(6):NP500-NP511. doi:10.1093/asj/sjaa220PubMedGoogle ScholarCrossref
41.Bravo BSF, Carvalho RM, Gallo BF, Bravo LG. A retrospective study supporting the importance of individualizing the dose of botulinum toxin according to the age. J Cutan Aesthet Surg. 2021;14(1):88-92. doi:10.4103/JCAS.JCAS_20_20PubMedGoogle ScholarCrossref
42.Joseph JH, Eaton LL, Robinson J, Pontius A, Williams EF III. Does increasing the dose of abobotulinumtoxina impact the duration of effectiveness for the treatment of moderate to severe glabellar lines? J Drugs Dermatol. 2016;15(12):1544-1549.PubMedGoogle Scholar
43.Hexsel D, Soirefmann M, Porto MD, Siega C, Schilling-Souza J, Rodrigues TC. Fields of muscular and anhidrotic effects of 2 botulinum toxin-A commercial preparations: a prospective, double-blind, randomized, multicenter study. Dermatol Surg. 2015;41(suppl 1):S110-S118. doi:10.1097/01.DSS.0000452645.76270.88PubMedGoogle ScholarCrossref
44.Yoo KH, Lee YW, Lee JS, Kwon SH, Huh CH, Kim BJ. Efficacy and safety of a new botulinum toxin (HU-014) versus existing onabotulinumtoxin A in subjects with moderate to severe glabellar lines. Dermatol Surg. 2021;47(3):e91-e96. doi:10.1097/DSS.0000000000002789PubMedGoogle ScholarCrossref
45.Branford OA, Dann SC, Grobbelaar AO. The quantitative assessment of wrinkle depth: turning the microscope on botulinum toxin type A. Ann Plast Surg. 2010;65(3):285-293. doi:10.1097/SAP.0b013e3181cbfee6PubMedGoogle ScholarCrossref
46.Sirisuthivoranunt S, Wongdama S, Phumariyapong P, et al. Comparative study on the duration and efficacy of various botulinum toxin type A injections for reducing masseteric muscle bite force and treating facial wrinkles. Dermatol Ther (Heidelb). 2024;14(5):1315-1325. doi:10.1007/s13555-024-01177-1PubMedGoogle ScholarCrossref
47.Fagien S, Avelar RL, Cox SE, Joseph JH, Kaufman-Janette J, Marcus KA. Safety and duration of effect of 40-unit prabotulinumtoxinA-xvfs for the treatment of moderate to severe glabellar lines in adult patients: a phase II, multicenter, randomized, double-blind, active-controlled trial. Aesthet Surg J. 2024;44(9):987-1000. doi:10.1093/asj/sjae051PubMedGoogle ScholarCrossref
48.Rupp DC, Canty D, Rhéaume C, et al. A preclinical study comparing the activity and potency of onabotulinumtoxina and prabotulinumtoxina. Clin Cosmet Investig Dermatol. 2023;16:581-591. doi:10.2147/CCID.S397999PubMedGoogle ScholarCrossref
49.Solish N, Ascher B, Avelar RL, et al. PrabotulinumtoxinA vs onabotulinumtoxinA for the treatment of adult males with moderate to severe glabellar lines: post-hoc analyses of the phase III clinical study data. Aesthet Surg J. 2022;42(12):1460-1469. doi:10.1093/asj/sjac210PubMedGoogle ScholarCrossref
50.Won CH, Kim HK, Kim BJ, et al. Comparative trial of a novel botulinum neurotoxin type A versus onabotulinumtoxinA in the treatment of glabellar lines: a multicenter, randomized, double-blind, active-controlled study. Int J Dermatol. 2015;54(2):227-234. doi:10.1111/ijd.12627PubMedGoogle ScholarCrossref
51.Gubanova E, Haddad Tabet M, Bergerova Y, et al. Assessment of subject and physician satisfaction after long-term treatment of glabellar lines with abobotulinumtoxinA (Dysport/Azzalure): primary results of the APPEAL noninterventional study. Aesthetic Plast Surg. 2018;42(6):1672-1680. doi:10.1007/s00266-018-1200-4PubMedGoogle ScholarCrossref
52.Molina B, Grangier Y, Mole B, et al. Patient satisfaction after the treatment of glabellar lines with Botulinum toxin type A (Speywood unit): a multi-centre European observational study. J Eur Acad Dermatol Venereol. 2015;29(7):1382-1388. doi:10.1111/jdv.12881PubMedGoogle ScholarCrossref
53.Schlessinger J, Cohen JL, Shamban A, et al. A multicenter study to evaluate subject satisfaction with two treatments of abobotulinumtoxina a year in the glabellar lines. Dermatol Surg. 2021;47(4):504-509. doi:10.1097/DSS.0000000000002846PubMedGoogle ScholarCrossref
54.Sobanko JF, Dai J, Gelfand JM, Sarwer DB, Percec I. Prospective cohort study investigating changes in body image, quality of life, and self-esteem following minimally invasive cosmetic procedures. Dermatol Surg. 2018;44(8):1121-1128. doi:10.1097/DSS.0000000000001523PubMedGoogle ScholarCrossref
55.Ascher B, Rzany B, Kestemont P, et al. Significantly increased patient satisfaction following liquid formulation abobotulinumtoxinA treatment in glabellar lines: FACE-Q outcomes from a phase 3 clinical trial. Aesthet Surg J. 2020;40(9):1000-1008. doi:10.1093/asj/sjz248PubMedGoogle ScholarCrossref
56.Farashi F, Ghoncheh M, Ghasemian Moghaddam MR, Soroosh Z. Evaluation of people’s satisfaction with botulinum toxin injection for facial rejuvenation based on age. J Cosmet Dermatol. 2024;23(7):2380-2385. doi:10.1111/jocd.16289PubMedGoogle ScholarCrossref
57.Lim JTE, Loh DKT, Soh K, Sunga O. Efficacy and patient satisfaction with incobotulinumtoxinA for the treatment of glabellar frown lines. Singapore Med J. 2017;58(10):606-609. doi:10.11622/smedj.2016112PubMedGoogle ScholarCrossref
58.Hexsel D, Cartier H, Hedén P, et al. Efficacy, safety, and subject satisfaction after abobotulinumtoxina treatment of upper facial lines. Dermatol Surg. 2018;44(12):1555-1564. doi:10.1097/DSS.0000000000001679PubMedGoogle ScholarCrossref
59.de Almeida ART, da Costa Marques ERM, Banegas R, Kadunc BV. Glabellar contraction patterns: a tool to optimize botulinum toxin treatment. Dermatol Surg. 2012;38(9):1506-1515. doi:10.1111/j.1524-4725.2012.02505.xPubMedGoogle ScholarCrossref