Treatment of androgenetic alopecia (AGA) with Sabal serrulata and biomimetic peptides delivered with microneedling
Enrique Lorente, Fabiola León Morales, María Llanos Pérez González
MEDICINA ESTÉTICA – Nº 68 – 3rd Quarter – 2021 | ISSN 1698-8337 | September 15, 2021
ABSTRACT
Introduction. Microneedling is a minimally invasive technique that allows the opening of microchannels in the skin, favoring the topical absorption of sterile medical and/or cosmetic preparations. Its use has spread in the treatment of different pathologies, including androgenetic alopecia (AGA).
The aim of the study is to assess the efficacy of microneedling in the treatment of AGA, by serial micropuncture, with commercially available sterile cosmetic preparations.
Material and Method. Ten male volunteer patients diagnosed with AGA, accentuated by the stress of the coronavirus pandemic (SARS-CoV-2), were included in the study. They underwent 10 treatment sessions performed weekly, using the microneedling technique followed by the application of 2 sterile topical cosmetic products containing Sabal serrulata and biomimetic growth factors. Daily home treatment with topical lotion and intake of a nutritional supplement was also prescribed.
Results. At the 5th session, a reduction in hair loss was observed in all patients. 60% presented a decrease in AGA on the Sinclair scale compared to the beginning of treatment, which was confirmed by trichogram. At the 10th session, 70% of the treated patients presented an improvement in cumulative hair thickness (mm/cm2).
Conclusions. Despite the limited number of patients, the transcutaneous administration of sterile topical cosmetics by microneedling together with home treatment may represent a successful approach to androgenetic alopecia.
Keywords. Androgenetic alopecia, microneedling, sterile cosmetics, Sabal serrulata, biomimetic peptides, nutritional supplements.
INTRODUCTION
Alopecia is the reversible or irreversible loss of previously existing hair follicles resulting in a decrease in hair density in a diffuse or localized manner [1]. Alopecia can be classified in various ways according to its origin and manifestations, the most common being androgenetic alopecia (AGA), commonly known as common baldness. This type of alopecia accounts for 95% of diagnoses made in clinical practice and is predominant in the Caucasian race. It affects up to 80% of the general male population and 50% of the female population at some point in their lives, with its prevalence increasing with age [2]. Hair loss can affect self-esteem and lead to depression. The impact on quality of life and the high incidence of AGA make it the most frequent reason for consultation in trichology [3].
AGA is a pathology with a genetic basis, variable penetrance and hormonal pathophysiology, which produces a progressive miniaturization of the scalp follicles, mainly in the frontal, parietal and temporal areas [1]. Genetic predisposition to alopecia accounts for 80% of existing cases [4]; genetic polymorphism explains the different ages of onset and degrees of presentation of AGA [5]. Follicular miniaturization represents a response of hair follicle cells to the rate of circulating androgens in the blood, in individuals with genetic predisposition, even when this rate is normal [6].
Testosterone is metabolized into dihydrotestosterone (DHT) by the enzyme 5-alpha reductase (5-αR), in its isoenzyme 1 and isoenzyme 2 forms. DHT has a high affinity for the androgenic receptors of the hair bulb and is considered the main factor responsible for androgen-mediated effects on the scalp of patients with AGA [7]. Under the influence of androgens, the dermal papilla of hair follicles secretes a significant amount of cytokines, such as TGF β-1, IL-1 α and TNFα, which can contribute to the shortening of the anagen phase [7].
Follicular miniaturization is a theory that explains the decrease in scalp density affected by AGA, which involves the shortening of the anagen phase in the hair cycle, and an ascent of the follicle from the reticular dermis to the papillary dermis that occurs progressively with each new hair cycle. Follicular units, previously larger and with terminal hairs, shrink and exhibit a vellus hair pattern [8]. It also explains the decrease in scalp density affected by AGA.
A large number of molecular signals are involved in the phases of the normal hair cycle. The transition from telogen to anagen follicles is associated with the activation of the Wnt/β-catenin/LEF-1 (Lymphoid enhancer-binding factor 1) signaling pathways, the exogenous Sonic Hedgehog (Shh) proteins and the STAT3 mediator proteins that act as mediators in gene expression in response to certain cellular stimuli, in addition to the downregulation of bone morphogenetic protein (BMP) signaling. The BMP-4 growth factor also appears to play an important role in the suppression of follicular growth and differentiation during the telogen phase. In AGA, circulating androgens enter the follicle through the capillaries of the dermal papilla (DP), bind to the androgen receptor within DP cells and then activate or repress the molecular signaling pathways responsible for premature anagen-to-catagen transition and follicular miniaturization. This includes the suppression of the stimulating pathways of Wnt, STAT3 and Shh, and the upregulation of suppressive pathways such as BMP [8–10].
Another explanation for the decrease in hair density is the increased duration of the kenogen phase, which can occur together with the miniaturization process. This is the so-called empty follicle phase that follows an exogenous event causing hair loss. This kenogen phase can last from 3 months to a year, but in AGA cases it may be longer [10]. An increase in follicles in this phase may be more important for the decrease in hair count than miniaturized hair follicles. Rushton et al. concluded that, after 12 months of AGA treatment, hair regrows more through the conversion of follicles from kenogen to anagen than through increased activity in miniaturized hair follicles [11].
Although the pathophysiology of AGA is closely related to androgen metabolism, scientific evidence suggests that it is also associated with dysregulation in the expression of inflammatory cytokines, with the consequent chronic microinflammation that acts as an aggravating factor in alopecia [12]. This inflammatory scenario can be caused by both endogenous and exogenous factors: endogenous bacterial flora in cases associated with seborrhea, oxidative stress, aging, smoking, ultraviolet radiation and pollutants [8]. Regarding exogenous factors, lifestyle modification can potentially reduce the extent of clinical manifestations [7].
The use of the microneedling technique has undergone significant evolution in recent years, allowing it to be introduced into the therapeutic arsenal as a low-cost tool with a low learning curve, comfortable for the patient and minimally invasive [9, 13–16].
The device uses a single-use head with a specific number of solid fine needles, connected to a motor that produces the rotation of this head and consequently facilitates skin micropunctures that generate microchannels crossing the outer layer of the skin, allowing the passage of small molecules of active substances. These micropunctures also stimulate neocollagenesis, neovascularization, expression of Wnt proteins and the release of growth factors [17–19]. Microneedling can be used as an adjuvant treatment for AGA, associated with other light-based, physical or cosmetic techniques, with an excellent safety profile [20].
Currently, the first-line treatments for AGA in males are oral anti-androgen drugs, inhibitors of 5-α reductase: dutasteride and finasteride. Dutasteride is the preferred choice as it inhibits both isoenzymes of 5-α reductase, while finasteride inhibits only isoenzyme type 2. In different clinical trials, dutasteride has shown a safety profile similar to finasteride, with greater clinical efficacy [21]. Likewise, Sabal serrulata has the ability to inhibit both isoenzymes of 5-α reductase in human prostatic tissue [22], although other studies have shown that oral intake of Sabal serrulata and certain nutritional supplements could increase the number of hairs in patients with AGA [23, 24].
The objective of this study is to verify the efficacy and safety of transdermal treatment of already commercially available sterile cosmetic preparations delivered through microneedling.
MATERIAL AND METHOD
The study was carried out following the principles established in the Declaration of Helsinki, updated in 2013. It is a prospective study on the efficacy and safety of the combined use of microneedling and the subsequent application of topical preparations. Ten male volunteer patients, previously diagnosed with AGA, with an average age of 46 years (range: 34–57), with a Sinclair scale score of 3.9 to 2.06, were enrolled. The study period was from September 2020 to December of the same year and was carried out at the ToskaniMed Medical Unit, Barcelona.
The following inclusion criteria were considered:
- Diagnosis of AGA of no less than 3 years.
- Greater hair loss during the confinement months, from March to May 2020.
- No treatment for AGA in the 6 months prior to the study.
- Absence of known allergies.
- Negative PCR and antigen tests during the study and its development.
- Acceptance, understanding and signing of the specific informed consent.
- Explicit commitment to carry out the recommended home treatment.
Materials used
A microneedling device (Neopen® Toskanimed, Equipmed USA LLC, Newport Beach, USA), equipped with a head of 16 solid 33G caliber steel needles, was used. Trichoscopy, for obtaining images of the scalp and hair, was performed using the dermatoscopic equipment Handyscope® (FotoFinder Systems GmbH, Bad Birnbach, Germany).
The trichoscopy images obtained were analyzed by the independent company TrichoLAB®, specialized in the analysis of trichological images, following the measurement protocol designed by them, which uses the Sinclair scale as a reference for the evolution of AGA. This avoided the subjective perception of the investigators.
Photographs were taken with a high-resolution imaging equipment (VisioFace® RD, Courage + Khazaka electronic GmbH, Cologne, Germany), before starting treatment and after the 5th and 10th sessions. To ensure the reproducibility of the images obtained from the study area, the equipment offers the option of superimposing images taken in the last session with those of the current session. It also has a homogeneous lighting system that ensures the photographic shots have the same lighting conditions in all captures.
The sterile cosmetic products used were (Hair Cocktail Plus®, Toskani, SL, Barcelona, Spain) and their composition is detailed below:
- Vial No. 1. (Hair Cocktail Plus® 10 ml, Toskani, SL, Barcelona, Spain) composed of:
- Sabal serrulata, inhibitor of both isoenzymes of 5αR.
- Coumarin and troxerutin, which stimulate microcirculation favoring the arrival of micronutrients to the follicle and hair bulb.
- Vitamins B6 and B8, with anti-seborrheic action.
- Glutathione, as an enzymatic activator.
- Panthenol, with anti-inflammatory action.
- Vial No. 2. (HCPR® 5 ml, Toskani, SL, Barcelona, Spain) composed of:
- Biomimetic peptides, which prolong the anagen phase and shorten the telogen phase.
- bFGF (basic fibroblast growth factor), which promotes blood microcirculation in the scalp.
- IGF-1 (insulin-like growth factor-1), which strengthens hair by stimulating hair follicles.
- VEGF (vascular endothelial growth factor), which promotes local angiogenesis.
- Minerals (sodium, potassium, magnesium and iron).
- Amino acids and vitamins A, B group, C, E and K, as micronutrients that stimulate regeneration and strengthen hair.
- Pre-treatment preparation did not require topical local anesthetics; disinfection was performed with chlorhexidine digluconate (Cristalmina® 1%, Laboratorios Salvat, Esplugues de Llobregat, Barcelona).
The treatment protocol in each weekly session was performed by separating the hair into longitudinal lines, sliding the device head twice, first in the occipito-frontal direction and then fronto-occipital. The needle head was adjusted to a depth of 1 mm and the rotation speed was set at 7,200 rpm. No bleeding was caused, only erythema. In the first 6 treatment sessions vial 1 was used, and from sessions 7 to 10 vial 2 was used. After each procedure, no aftercare was necessary, except that patients should not shower in the following 8–10 hours or bathe at the beach or pool. All patients were able to resume their daily activities.
Three high-definition trichoscopies were performed before the start of treatment (T0), after the 5th session (T5), and after the 10th session (T10), in each of the following areas: middle frontal area, 2 cm behind the hairline; left temporal area, 3 cm above the ear canal, and at the occipital protuberance. The objective variables provided by the trichoscopies were evaluated by the independent laboratory TrichoLAB®. The following variables were considered:
- Average number of hairs per control area [N/cm2].
- Average hair shaft thickness [µm].
- Cumulative hair thickness per surface area [mm/cm2].
- Sinclair scale.
The home treatment consisted of:
- Topical lotion (Anti Hair-loss lotion®, Toskani, SL, Barcelona, Spain). One application every night consisting of 7 sprays. Its composition includes:
- Sabal serrulata.
- Aminexil, with a vasodilatory effect similar to minoxidil and collagen regeneration.
- Zinc, stimulator of hair growth.
- Oral treatment (Densihair Boost Capsules®, Toskani, SL, Barcelona, Spain). 2 capsules per day were recommended, whose composition is: Sabal serrulata, zinc, selenium, biotin, lysine, cystine and arginine.
Upon completion of treatment, a survey was conducted with all volunteers to determine their degree of satisfaction.
Statistical analysis. Data were expressed as mean ± standard deviation. A normality analysis of the sample was performed using the Shapiro-Wilk test and the non-parametric Wilcoxon test was applied to compare results between all study areas and with baseline status. Statistical analyses were performed using SPSS v.20 (IBM, Madrid, Spain). A p value < 0.05 was considered to indicate statistical significance.
Participant satisfaction data were obtained through individual surveys and expressed as percentages.
The statistical study of the trichological analysis was performed by Tricholab System® based on the Trichoscopy Derived Sinclair Scale.
RESULTS
All recruited patients completed the study. No volunteer showed adverse effects during or after treatment. Side effects were those intrinsic to the micropuncture technique, being labeled as mild and transient: erythema and mild discomfort during the procedure.
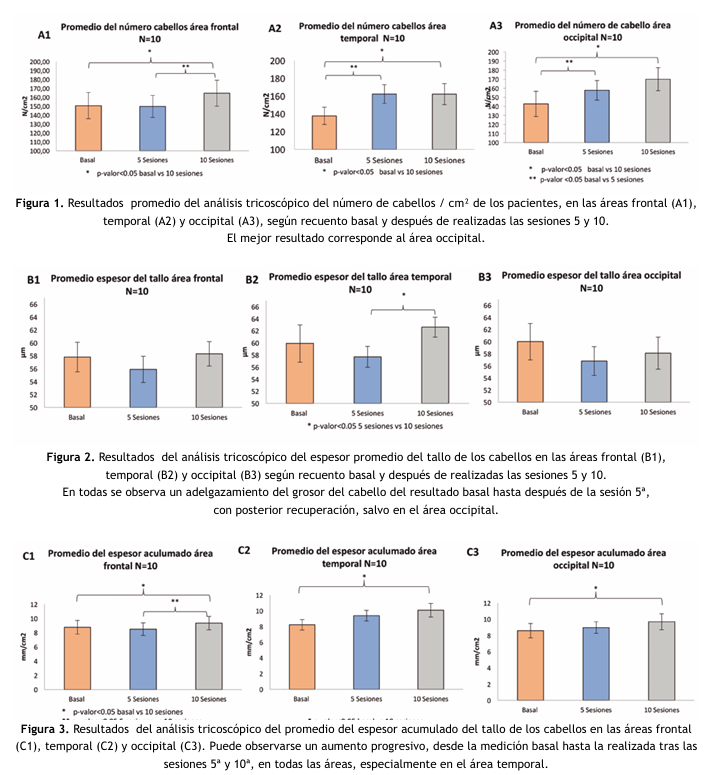
- The number of hairs per area (N/cm2) was recorded in the frontal, temporal and occipital areas. The best result was obtained in the occipital area with an average of 16.9% (p = 0.005) compared to the baseline measurement. In the frontal and temporal areas, less significant average improvements of 11.7% (p = 0.036) and 8.67% (p = 0.047) were obtained respectively (Figure 1). The overall degree of improvement across all patients was 40%.
- The result of measuring hair shaft thickness, expressed in µm, in the same areas showed thinning in all areas from the initial baseline measurement to that taken after the 5th session, being greatest in the occipital area (3.4%). Shaft thickness recovered in all areas after the measurement following the 10th session: increasing 0.7% in the frontal area, 4.4% in the temporal and 0.5% in the occipital (Figure 2).
The overall percentage of improvement in patients, from the baseline measurement to that obtained after the 10th session, was: 60% in the frontal area, 70% in the temporal and 40% in the occipital.
- In cumulative hair thickness (mm/cm2), an improvement at the end of treatment was observed of 6.8% (p = 0.048) in 40% of patients in the frontal area; of 14.7% (p = 0.044) in 70% of patients in the temporal area, and of 10.5% (p = 0.046) in 69% in the occipital area (Figure 3).
- The evolution of AGA according to the Sinclair scale, measured with TrichoLAB® technology comparing the baseline state and after completing the 10 sessions, was as follows: a. In the frontal area, 30% of patients achieved significant improvement, while 40% showed no changes and the remaining 30% worsened slightly (estimated at 1.23%). Overall, the average improvement went from 2.7 ± 0.2 at baseline to 2.8 ± 0.1 at the end of treatment. b. In the temporal area, only 40% of patients showed improvement while 60% experienced worsening compared to the initial study. The average baseline status went from 2.7 ± 0.1 to 2.6 ± 0.1 at the final state. c. In the occipital area, 60% of those treated experienced a degree of improvement and 40% had a slight worsening (estimated at 1.1%). The average baseline status went from 2.7 ± 0.2 to 2.7 ± 0.3 at the final state.
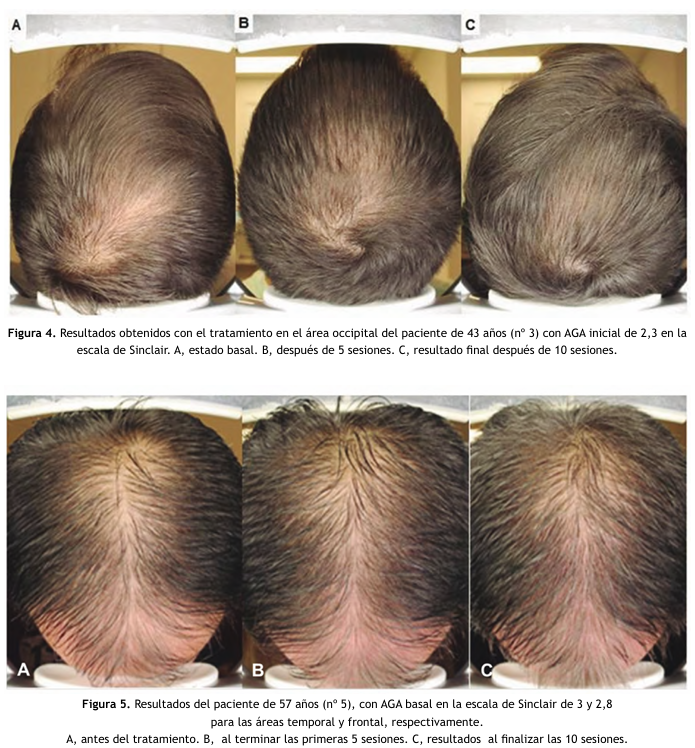
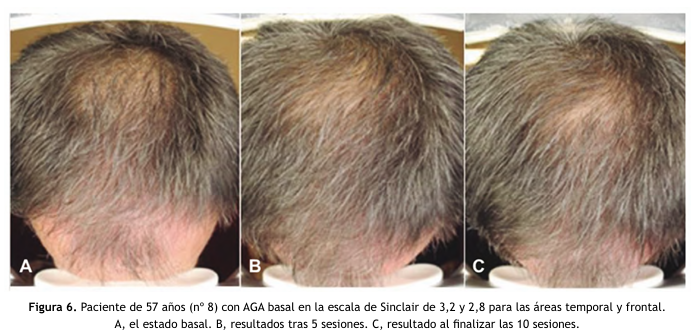
Figures 4, 5 and 6 show details of the results achieved, before starting treatment and after completing 5 and 10 sessions, in 3 of the 10 treated patients.
The patients’ assessment of the results achieved was as follows:
a. All patients felt satisfied with the results obtained. b. Regarding their perception of the anti-hair loss effect of the treatment, 50% of volunteers noticed an intense improvement; 40% of participants rated it as moderate, and the remaining 10% answered that it was slight. c. Regarding hair density, 20% of respondents reported noticing an intense improvement, 50% as moderate and the remaining 30% as slight. d. Finally, regarding the appearance of new hair, 60% of participants noticed a moderate improvement; 30% detected a slight improvement and the remaining 10% identified no improvement at all.
DISCUSSION
AGA is characterized by a progressive reduction in the diameter, length and pigmentation of hair, in both men and women, generating problems that are not only aesthetic but also emotional [3]. Despite the existing social demand, currently only two drugs are approved by the FDA for the treatment of AGA: topical minoxidil and finasteride [25]. However, some studies on the combination of the microneedling technique with minoxidil [16] have shown greater effectiveness than the use of minoxidil alone, reinforcing the hypothesis that microneedling favors the penetration of active ingredients while enhancing neovascularization [26]. On the other hand, treatments based on the inhibition of the action of 5-α reductase, finasteride and dutasteride, are effective in the treatment of AGA, although they are not without controversial adverse effects that limit or advise against their use [27].
For this reason, studies are being carried out based on natural-origin extracts that exhibit 5-α reductase inhibitory properties, such as Sabal serrulata, with the potential to be effective in the treatment of AGA. Among its advantages is that it is well tolerated in humans and can be administered orally and topically; in the latter case, with the help of microneedling for greater efficacy of its absorption and therapeutic response, thus opening a wide range of possibilities for the treatment of AGA. Without forgetting that not only hormonal factors contribute to the etiopathogenesis of AGA — the contribution of inflammatory and oxidative factors must also be kept in mind [27].
For the present study, a treatment protocol was devised that addressed these three pathways involved in the etiopathogenesis of AGA; using, firstly, the microneedling technique to deliver the active ingredients contained in commercially available sterile cosmetic vials (Vials No. 1 and No. 2), supplemented with a topical lotion and a food supplement prescribed to all patients, forming part of the standardized protocol for all volunteers.
Taking into account the typical male pattern of hair loss, with greater loss in certain areas, especially frontal and occipital, the results have shown particularly notable efficacy in the occipital area, being moderate-slight in the frontal area, consistent with the hypothesis that the combination of treatments based on Sabal serrulata and biomimetic peptides combined with the action of serial micropuncture, which favors the penetration of these molecules while improving the microcirculation of the area [8]. The analyzed results show that hair loss has been slowed, with an increase in the number of new hairs and an increase in cumulative thickness [28].
A significant increase in hair shaft thickness has also been observed in both the frontal and temporal areas, being lesser in the occipital area. The decrease in hair shaft thickness in this area has been interpreted in relation to the appearance of new hairs in this area.
The non-uniform response in the different areas may be conditioned by the short follow-up period, which we consider one of the limitations of the present study. Therefore, it is advisable to undertake new studies with longer follow-up periods in order to observe late responses to treatment and verify the duration of the results obtained. Long-term follow-up controls are necessary, which will ultimately allow better adjustment of the frequency of future sessions.
Likewise, although the number of cases included in the study is limited, both the result achieved and the degree of satisfaction expressed by patients showed that the treatment had met the expectations of the volunteers in all cases. The number of sessions performed is consistent with the efficacy observed in terms of reduction of hair loss, the safety of the active ingredients and the microneedling technique used.
CONCLUSIONS
The transcutaneous administration of sterile cosmetics for topical use, delivered with microneedling, is a promising technique that shows evidence of reduction in hair loss and growth of new hairs.
The side effects observed during treatment were limited to the appearance of erythema, accompanied by short-duration itching in the treated area. Therefore, the treatment is considered effective, safe and is accompanied by a high degree of patient satisfaction.
Conflict of interest
ToskaniMed laboratory provided the products and the use of its facilities to carry out the treatments used in this study.
BIBLIOGRAFÍA
(1). Camacho Martínez, Francisco Miguel (Editor/a), Tosti, Antonella (Editor/a), Randall, Valerie E.
(Coeditor/a), Price, Vera H. (Coeditor/a): Montagna Tricología. Enfermedades del folículo piloso
(Tercera Edición). Grupo Aula Médica. 2013.
(2). Tosti A. Dermoscopy of hair and nail disorders. 2nd ed. CRC Press. Boca Raton, FL. 2015.
(3). N. Hunt, S. McHale. Hunt N, McHale S. The psychological impact of alopecia. BMJ. 2005 Oct
22;331(7522):951-3.
(4). Katzer T, Leite Junior A, Beck R, da Silva C. Physiopathology and current treatments of androgenetic
alopecia: Going beyond androgens and anti-androgens. Dermatol Ther. 2019 Sep;32(5):e13059.
(5). Hagenaars SP, Hill WD, Harris SE, Ritchie SJ, Davies G, Liewald DC, Gale CR, Porteous DJ, Deary IJ,
Marioni RE. Genetic prediction of male pattern baldness. PLoS Genet. 2017 Feb 14;13(2): e1006594.
(6). Gatherwright J, Liu MT, Amirlak B, Gliniak C, Totonchi A, Guyuron B. The contribution of endogenous
and exogenous factors to male alopecia: a study of identical twins. Plast Reconstr Surg. 2013
May;131(5):794e-801e.
(7). Rossi A, Anzalone A, Fortuna MC, Caro G, Garelli V, Pranteda G, Carlesimo M. Multi-therapies in
androgenetic alopecia: review and clinical experiences. Dermatol Ther. 2016 nov;29(6):424-432.
(8). Whiting DA. Possible mechanisms of miniaturization during androgenetic alopecia or pattern hair loss.
J Am Acad Dermatol. 2001 Sep;45(3 Suppl): S81-6.
TRATAMIENTO DE ALOPECIA ANDROGENÉTICA (AGA) CON SABAL SERRULATA Y PÉPTIDOS BIOMIMÉTICOS VEHICULIZADOS CON MICRONEEDLING
(9). Katzer T, Leite Junior A, Beck R, da Silva C. Physiopathology and current treatments of androgenetic
alopecia: Going beyond androgens and anti-androgens. Dermatol Ther. 2019 Sep;32(5):e13059.
(10). Kim YS, Jeong KH, Kim JE, Woo YJ, Kim BJ, Kang H. Repeated Microneedle Stimulation Induces Enhanced
Hair Growth in a Murine Model. Ann Dermatol. 2016 Oct;28(5):586-592.
(11). Guarrera M, Rebora A. Kenogen in female androgenetic alopecia. A longitudinal study. Dermatology.
2005;210(1):18-20.
(12). Hugh Rushton D, Norris MJ, Van Neste D. Hair regrowth in male and female pattern hair loss does not
involve the conversion of vellus hair to terminal hair. Exp Dermatol. 2016 Jun;25(6):482-4.
(13). Ramos PM, Brianezi G, Martins AC, da Silva MG, Marques ME, Miot HA. Apoptosis in follicles of
individuals with female pattern hair loss is associated with perifollicular microinflammation. Int J Cosmet
Sci. 2016 Dec;38(6):651-654.
(14). Kim BJ, Lim YY, Kim HM, et al. Hair follicle regeneration in mice after wounding by microneedle roller.
Int J Trichology. 2012;4:117.
(15). Kim YS, Jeong KH, Kim JE, Woo YJ, Kim BJ, Kang H. Repeated Microneedle Stimulation Induces Enhanced
Hair Growth in a Murine Model. Ann Dermatol. 2016 Oct;28(5):586-592.
(16). Jha AK, Udayan UK, Roy PK, Amar AKJ, Chaudhary RKP. Original article: Platelet-rich plasma with
microneedling in androgenetic alopecia along with dermoscopic pre- and post-treatment evaluation. J
Cosmet Dermatol. 2018 Jun;17(3):313-318.
(17). Dhurat R, Sukesh M, Avhad G, Dandale A, Pal A, Pund P. A randomized evaluator blinded study of effect
of microneedling in androgenetic alopecia: a pilot study. Int J Trichology. 2013 Jan;5(1):6-11.
(18). Faghihi G, Nabavinejad S, Mokhtari F, Fatemi Naeini F, Iraji F. Microneedling in androgenetic alopecia;
comparing two different depths of microneedles. J Cosmet Dermatol. 2021 Apr;20(4):1241-1247.
(19). Yang G, Chen G, Gu Z. Transdermal Drug Delivery for Hair Regrowth. Mol Pharm. 2021 Feb 1;18(2):483
(20). Willert K, Nusse R. Wnt proteins. Cold Spring Harb Perspect Biol. 2012 Sep 1;4(9):a007864.
(21). Vañó S. Jaen J. Manual práctico de Tricología. TricoHRC. Madrid. 2019.
(22). Di Silverio F, Monti S, Sciarra A, Varasano PA, Martini C, Lanzara S, D’Eramo G, Di Nicola S, Toscano
V. Effects of long-term treatment with Serenoa repens (Permixon) on the concentrations and regional
distribution of androgens and epidermal growth factor in benign prostatic hyperplasia. Prostate. 1998
Oct 1;37(2):77-83.
(23). Rossi A, Mari E, Scarno M, Garelli V, Maxia C, Scali E, Iorio A, Carlesimo M. Comparitive effectiveness
of finasteride vs Serenoa repens in male androgenetic alopecia: a two-year study. Int J Immunopathol
Pharmacol. 2012 Oct-Dec;25(4):1167-73.
(24). Morganti P, Fabrizi G, James B et al. Effect of gelatin-cystine and Serenoa repens extract on free radical
levels and hair growth. J. Appl. Cosmetol. 1998; 16: 57–64.
(25). Kelly Y, Blanco A, Tosti A. Androgenetic Alopecia: An Update of Treatment Options. Drugs. 2016
Sep;76(14):1349-64.
(26). Shah KB, Shah AN, Solanki RB, Raval RC. A Comparative Study of Microneedling with Platelet-rich
Plasma Plus Topical Minoxidil (5%) and Topical Minoxidil (5%) Alone in Androgenetic Alopecia. Int J
Trichology. 2017 Jan-Mar;9(1):14-18.
(27). Andriole GL, Kirby R. Safety and tolerability of the dual 5alpha-reductase inhibitor dutasteride in the
treatment of benign prostatic hyperplasia. Eur Urol. 2003 Jul;44(1):82-8.
(28). Guerra A, Gonzalez-Guerra, Borrás JM. Alopecia androgénica femenina. Nuevas herramientas
terapéuticas frente a los factores fisiopatológicos implicados: hormonal, oxidativo e inflamatorio. Más
Dermatología. 2017;27:21-33.
(29). Kasprzak M, Sicińska J, Sinclair R. The Trichoscopy Derived Sinclair Scale: Enhancing visual assessment
through quantitative trichoscopy. Australas J Dermatol. 2019 May;60(2):134-136.